Living With Severs Disease
Overview
Sever?s disease is a condition occurring in pre-adolescents that causes pain, swelling and soreness in the heel bone, also known as the calcaneus. Sever?s disease causes pain on either side of and/or on the bottom of the heel. During a period of pre-adolescent development, the growing heel bone can be overused when the child is involved in a lot of running and jumping activities. Impact on the heel bone and repeated traction on the growing bone from the Achilles tendon can lead to swelling in the area.
Causes
Predisposing Hereditary Factors: These are a biomechanical defect that one may be born with, which increases the chances of developing Sever's Disease. Short Achilles Tendon, When the Achilles Tendon is short from birth, it will exaggerate the tightness of this tendon that occurs during a child's growing years. This makes the pull of the Achilles Tendon on the heel's growth plate more forceful than normal, causing inflammation and pain, and eventually Sever's Disease. Short Leg Syndrome, When one leg is shorter than the other, the foot on the short leg must plantar flex (the foot and toes bend down) in order to reach the ground. In this way, the body tries to equalize the length of the legs. In order for the foot to plantar flex, the Achilles Tendon must pull on the heel with greater force than if the leg was a normal length. Thus the heel on the short leg will be more susceptible to Sever's Disease during the foot's growing years. Pronation. Is a biomechanical defect of the foot that involves a rolling outward of the foot at the ankle, so that when walking, the inner side of the heel and foot bears more of the body's weight than is normal (click here for more information about pronation). Pronation thus causes the heel to be tilted or twisted. In order for the Achilles Tendon to attach to the heel, it must twist to reach its normal attachment site. This will shorten or tighten the Achilles Tendon and increase the force of its pull on the heel's growth plate. This will increase the tightness of the Achilles Tendon during the foot's growing years, and may help to initiate bouts of Sever's Disease. Flat Arches and High Arches. Both of these biomechanical foot defects effect the pitch, or angle of the heel within the foot. When the heel is not positioned normally within the foot due to the height of the arch, the Achilles Tendon's attachment to the heel is affected. This may produce a shortening or tightening of the Achilles Tendon, which increases the force of its pull on the heel's growth plate. During the foot's growing years, abnormal arch height may contribute to the onset of Sever's Disease.
Symptoms
The typical patient is a child between 10 and 13 years of age, complaining of pain in one or both heels with running and walking. The pain is localized to the point of the heel where the tendo-achilles inserts into the calcaneus (heel bone), and is tender to deep pressure at that site. Walking on his toes relieves the pain.
Diagnosis
Sever condition is diagnosed by detecting the characteristic symptoms and signs above in the older children, particularly boys between 8 and 15 years of age. Sometimes X-ray testing can be helpful as it can occasionally demonstrate irregularity of the calcaneus bone at the point where the Achilles tendon attaches.
Non Surgical Treatment
Occasionally, an orthotic may need to be prescribed for temporary or long-term correction of their foot biomechanics (eg flat feet or high arches). During the acute phase of Sever's disease a small heel rise or shock-absorbing heel cup placed under the heel pad of your child's foot may help to ease the symptoms. Your podiatrist or physiotherapist can assess your child's arch and guide you in the best management of your child's condition. We recommend that your child should never go barefooted during the painful stages of Sever's disease.
Recovery
Although Sever's disease generally heals quickly, it can recur if long-term measures are not taken to protect the heel during a child's growing years. One of the most important is to make sure that kids wear proper shoes. Good quality, well-fitting shoes with shock-absorbent (padded) soles help to reduce pressure on the heel. The doctor may also recommend shoes with open backs, such as sandals or clogs, that do not rub on the back of the heel. Shoes that are heavy or have high heels should be avoided. Other preventive measures include continued stretching exercises and icing of the affected heel after activity.
Sever?s disease is a condition occurring in pre-adolescents that causes pain, swelling and soreness in the heel bone, also known as the calcaneus. Sever?s disease causes pain on either side of and/or on the bottom of the heel. During a period of pre-adolescent development, the growing heel bone can be overused when the child is involved in a lot of running and jumping activities. Impact on the heel bone and repeated traction on the growing bone from the Achilles tendon can lead to swelling in the area.
Causes
Predisposing Hereditary Factors: These are a biomechanical defect that one may be born with, which increases the chances of developing Sever's Disease. Short Achilles Tendon, When the Achilles Tendon is short from birth, it will exaggerate the tightness of this tendon that occurs during a child's growing years. This makes the pull of the Achilles Tendon on the heel's growth plate more forceful than normal, causing inflammation and pain, and eventually Sever's Disease. Short Leg Syndrome, When one leg is shorter than the other, the foot on the short leg must plantar flex (the foot and toes bend down) in order to reach the ground. In this way, the body tries to equalize the length of the legs. In order for the foot to plantar flex, the Achilles Tendon must pull on the heel with greater force than if the leg was a normal length. Thus the heel on the short leg will be more susceptible to Sever's Disease during the foot's growing years. Pronation. Is a biomechanical defect of the foot that involves a rolling outward of the foot at the ankle, so that when walking, the inner side of the heel and foot bears more of the body's weight than is normal (click here for more information about pronation). Pronation thus causes the heel to be tilted or twisted. In order for the Achilles Tendon to attach to the heel, it must twist to reach its normal attachment site. This will shorten or tighten the Achilles Tendon and increase the force of its pull on the heel's growth plate. This will increase the tightness of the Achilles Tendon during the foot's growing years, and may help to initiate bouts of Sever's Disease. Flat Arches and High Arches. Both of these biomechanical foot defects effect the pitch, or angle of the heel within the foot. When the heel is not positioned normally within the foot due to the height of the arch, the Achilles Tendon's attachment to the heel is affected. This may produce a shortening or tightening of the Achilles Tendon, which increases the force of its pull on the heel's growth plate. During the foot's growing years, abnormal arch height may contribute to the onset of Sever's Disease.
Symptoms
The typical patient is a child between 10 and 13 years of age, complaining of pain in one or both heels with running and walking. The pain is localized to the point of the heel where the tendo-achilles inserts into the calcaneus (heel bone), and is tender to deep pressure at that site. Walking on his toes relieves the pain.
Diagnosis
Sever condition is diagnosed by detecting the characteristic symptoms and signs above in the older children, particularly boys between 8 and 15 years of age. Sometimes X-ray testing can be helpful as it can occasionally demonstrate irregularity of the calcaneus bone at the point where the Achilles tendon attaches.
Non Surgical Treatment
Occasionally, an orthotic may need to be prescribed for temporary or long-term correction of their foot biomechanics (eg flat feet or high arches). During the acute phase of Sever's disease a small heel rise or shock-absorbing heel cup placed under the heel pad of your child's foot may help to ease the symptoms. Your podiatrist or physiotherapist can assess your child's arch and guide you in the best management of your child's condition. We recommend that your child should never go barefooted during the painful stages of Sever's disease.
Recovery
Although Sever's disease generally heals quickly, it can recur if long-term measures are not taken to protect the heel during a child's growing years. One of the most important is to make sure that kids wear proper shoes. Good quality, well-fitting shoes with shock-absorbent (padded) soles help to reduce pressure on the heel. The doctor may also recommend shoes with open backs, such as sandals or clogs, that do not rub on the back of the heel. Shoes that are heavy or have high heels should be avoided. Other preventive measures include continued stretching exercises and icing of the affected heel after activity.
The Causes Of Posterior Tibial Tendon Dysfunction ?
Overview
The posterior tibial tendon serves as one of the major supporting structures of the foot, helping it to function while walking. Posterior tibial tendon dysfunction (PTTD) is a condition caused by changes in the tendon, impairing its ability to support the arch. This results in flattening of the foot. PTTD is often called ?adult acquired flatfoot? because it is the most common type of flatfoot developed during adulthood. Although this condition typically occurs in only one foot, some people may develop it in both feet. PTTD is usually progressive, which means it will keep getting worse, especially if it isn?t treated early. 
Causes
Obesity - Overtime if your body is carrying those extra pounds, you can potentially injure your feet. The extra weight puts pressure on the ligaments that support your feet. Also being over weight can lead to type two diabetes which also can attribute to AAFD. Diabetes - Diabetes can also play a role in Adult Acquired Flatfoot Deformity. Diabetes can cause damage to ligaments, which support your feet and other bones in your body. In addition to damaged ligaments, uncontrolled diabetes can lead to ulcers on your feet. When the arches fall in the feet, the front of the foot is wider, and outer aspects of the foot can start to rub in your shoe wear. Patients with uncontrolled diabetes may not notice or have symptoms of pain due to nerve damage. Diabetic patient don?t see they have a problem, and other complications occur in the feet such as ulcers and wounds. Hypertension - High blood pressure cause arteries narrow overtime, which could decrease blood flow to ligaments. The blood flow to the ligaments is what keeps the foot arches healthy, and supportive. Arthritis - Arthritis can form in an old injury overtime this can lead to flatfeet as well. Arthritis is painful as well which contributes to the increased pain of AAFD. Injury - Injuries are a common reason as well for AAFD. Stress from impact sports. Ligament damage from injury can cause the bones of the foot to fallout of ailment. Overtime the ligaments will tear and result in complete flattening of feet.
Symptoms
Depending on the cause of the flatfoot, a patient may experience one or more of the different symptoms here. Pain along the course of the posterior tibial tendon which lies on the inside of the foot and ankle. This can be associated with swelling on the inside of the ankle. Pain that is worse with activity. High intensity or impact activities, such as running, can be very difficult. Some patients can have difficulty walking or even standing for long periods of time. When the foot collapses, the heel bone may shift position and put pressure on the outside ankle bone (fibula). This can cause pain on the outside of the ankle. Arthritis in the heel also causes this same type of pain. Patients with an old injury or arthritis in the middle of the foot can have painful, bony bumps on the top and inside of the foot. These make shoewear very difficult. Occasionally, the bony spurs are so large that they pinch the nerves which can result in numbness and tingling on the top of the foot and into the toes. Diabetics may only notice swelling or a large bump on the bottom of the foot. Because their sensation is affected, people with diabetes may not have any pain. The large bump can cause skin problems and an ulcer (a sore that does not heal) may develop if proper diabetic shoewear is not used.
Diagnosis
Looking at the patient when they stand will usually demonstrate a flatfoot deformity (marked flattening of the medial longitudinal arch). The front part of the foot (forefoot) is often splayed out to the side. This leads to the presence of a ?too many toes? sign. This sign is present when the toes can be seen from directly behind the patient. The gait is often somewhat flatfooted as the patient has the dysfunctional posterior tibial tendon can no longer stabilize the arch of the foot. The physician?s touch will often demonstrate tenderness and sometimes swelling over the inside of the ankle just below the bony prominence (the medial malleolus). There may also be pain in the outside aspect of the ankle. This pain originates from impingement or compression of two tendons between the outside ankle bone (fibula) and the heel bone (calcaneus) when the patient is standing.
Non surgical Treatment
Orthotic or anklebrace, Over-the-counter or custom shoe inserts to position the foot and relieve pain are the most common non-surgical treatment option. Custom orthotics are often suggested if the shape change of the foot is more severe. An ankle brace (either over-the-counter or custom made) is another option that will help to ease tendon tension and pain. Boot immobilization. A walking boot supports the tendon and allows it to heal. Activity modifications. Depending on what we find, we may recommend limiting high-impact activities, such as running, jumping or court sports, or switching out high-impact activities for low-impact options for a period of time. Ice and anti-inflammatory medications. These may be given as needed to decrease your symptoms. 
Surgical Treatment
In cases where cast immobilization, orthoses and shoe therapy have failed, surgery is the next alternative. The goal of surgery and non-surgical treatment is to eliminate pain, stop progression of the deformity and improve mobility of the patient. Opinions vary as to the best surgical treatment for adult acquired flatfoot. Procedures commonly used to correct the condition include tendon debridement, tendon transfers, osteotomies (cutting and repositioning of bone) and joint fusions. (See surgical correction of adult acquired flatfoot). Patients with adult acquired flatfoot are advised to discuss thoroughly the benefits vs. risks of all surgical options. Most procedures have long-term recovery mandating that the correct procedure be utilized to give the best long-term benefit. Most flatfoot surgical procedures require six to twelve weeks of cast immobilization. Joint fusion procedures require eight weeks of non-weightbearing on the operated foot - meaning you will be on crutches for two months. The bottom line is, Make sure all of your non-surgical options have been covered before considering surgery. Your primary goals with any treatment are to eliminate pain and improve mobility. In many cases, with the properly designed foot orthosis or ankle brace, these goals can be achieved without surgical intervention.
What Can Cause Heel Soreness
Overview

Heel pain is unlike most body aches and injuries because heels can't be immobilized to rest and recover, at least without considerable inconvenience to the sufferer. Heels can?t be isolated and splinted either ,as body weight will continue to aggravate the condition with every step. Heel pain can be devastating if left untreated, eventually impairing the ability to walk comfortably-or at all. Most Heel Pain comes from tendon problems, though some types can come from bone issues as well.
Causes
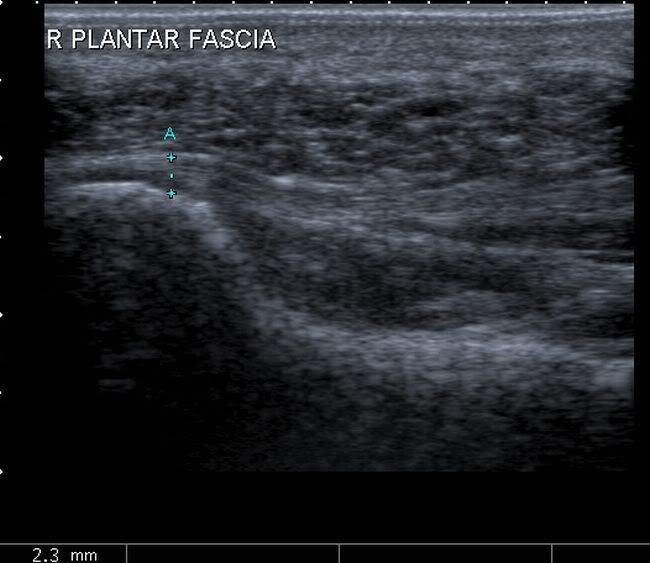
The plantar fascia spans the long arch of the foot from the heel to the base of the toes, where it blends with the soft tissues, then anchoring to the base of the toes. Plantar Fascia. The plantar fascia is a common cause of heel pain. As the bony attachment at the heel is considered the plantar fascia?s ?weak spot?, the patient will present with pain at the heel, mainly on the inside. The most common predisposing factor to this condition is the pronating (flattening feet) - 52% - whilst there is also some evidence that a very high arch, in a rigid foot (pes cavus), also was reasonably common - 42%.
Symptoms
Both heel pain and heel spurs are frequently associated with an inflammation of the long band of tissue that connects the heel and the ball of the foot. The inflammation of this arch area is called plantar fasciitis. The inflammation maybe aggravated by shoes that lack appropriate support and by the chronic irritation that sometimes accompanies an athletic lifestyle. Achilles Tendinopathy, Pain and inflammation of the tendon at the back of the heel that connects the calf muscle to the foot. Sever?s, Often found in children between the ages of 8 - 13 years and is an inflammation of the calcaneal epiphyseal plate (growth plate) in the back of the heel. Bursitis, An inflamed bursa is a small irritated sack of fluid at the back of the heel. Other types of heel pain include soft tissue growths, Haglunds deformity (bone enlargement at the back of the heel), bruises or stress fractures and possible nerve entrapment.
Diagnosis
Your doctor will listen to your complaints about your heel and examine you to see what is causing the pain, and whether anything else has started it off. If the cause of your pain seems obvious, your doctor may be happy to start treatment straight away. However, some tests may be helpful in ruling out other problems. Blood tests may be done for arthritis. An Xray will show any arthritis in the ankle or subtalar joint, as well as any fracture or cyst in the calcaneum. (It will also show a spur if you have one, but as we know this is not the cause of the pain.) Occasionally a scan may be used to help spot arthritis or a stress fracture.
Non Surgical Treatment
If you develop heel pain, you can try several methods at home to ease your discomfort. For example rest as much as possible, apply ice to the heel for 10 to 15 minutes twice a day, use over-the-counter pain medications, wear shoes that fit properly, wear night splints, a special device that stretches the foot while you sleep, use heel cups or shoe inserts to reduce pain, If these home care strategies do not ease your pain, you will need to see your doctor. He or she will perform a physical exam and ask you about your symptoms and when they began. Your doctor may also take an X-ray to determine the cause of your heel pain. Once your doctor knows what is causing your pain, he or she will be able to provide you with the appropriate treatment. In many cases, your doctor may prescribe physical therapy. This can help to strengthen the muscles and tendons in your foot, which helps to prevent further injury. If your pain is severe, your doctor may provide you with anti-inflammatory medications. These medications can be injected into the foot or taken by mouth. Your doctor may also recommend that you support your foot as much as possible-either by taping the foot or by using special footwear devices. In very rare cases, your doctor may recommend surgery to correct the problem. However, heel surgery often requires a long recovery time and may not always relieve your foot pain.
Surgical Treatment
Surgery to correct heel pain is generally only recommended if orthotic treatment has failed. There are some exceptions to this course of treatment and it is up to you and your doctor to determine the most appropriate course of treatment. Following surgical treatment to correct heel pain the patient will generally have to continue the use of orthotics. The surgery does not correct the cause of the heel pain. The surgery will eliminate the pain but the process that caused the pain will continue without the use of orthotics. If orthotics have been prescribed prior to surgery they generally do not have to be remade.
Prevention

Maintaining flexible and strong muscles in your calves, ankles, and feet can help prevent some types of heel pain. Always stretch and warm-up before exercising. Wear comfortable, properly fitting shoes with good arch support and cushioning. Make sure there is enough room for your toes.
Heel pain is unlike most body aches and injuries because heels can't be immobilized to rest and recover, at least without considerable inconvenience to the sufferer. Heels can?t be isolated and splinted either ,as body weight will continue to aggravate the condition with every step. Heel pain can be devastating if left untreated, eventually impairing the ability to walk comfortably-or at all. Most Heel Pain comes from tendon problems, though some types can come from bone issues as well.
Causes
The plantar fascia spans the long arch of the foot from the heel to the base of the toes, where it blends with the soft tissues, then anchoring to the base of the toes. Plantar Fascia. The plantar fascia is a common cause of heel pain. As the bony attachment at the heel is considered the plantar fascia?s ?weak spot?, the patient will present with pain at the heel, mainly on the inside. The most common predisposing factor to this condition is the pronating (flattening feet) - 52% - whilst there is also some evidence that a very high arch, in a rigid foot (pes cavus), also was reasonably common - 42%.
Symptoms
Both heel pain and heel spurs are frequently associated with an inflammation of the long band of tissue that connects the heel and the ball of the foot. The inflammation of this arch area is called plantar fasciitis. The inflammation maybe aggravated by shoes that lack appropriate support and by the chronic irritation that sometimes accompanies an athletic lifestyle. Achilles Tendinopathy, Pain and inflammation of the tendon at the back of the heel that connects the calf muscle to the foot. Sever?s, Often found in children between the ages of 8 - 13 years and is an inflammation of the calcaneal epiphyseal plate (growth plate) in the back of the heel. Bursitis, An inflamed bursa is a small irritated sack of fluid at the back of the heel. Other types of heel pain include soft tissue growths, Haglunds deformity (bone enlargement at the back of the heel), bruises or stress fractures and possible nerve entrapment.
Diagnosis
Your doctor will listen to your complaints about your heel and examine you to see what is causing the pain, and whether anything else has started it off. If the cause of your pain seems obvious, your doctor may be happy to start treatment straight away. However, some tests may be helpful in ruling out other problems. Blood tests may be done for arthritis. An Xray will show any arthritis in the ankle or subtalar joint, as well as any fracture or cyst in the calcaneum. (It will also show a spur if you have one, but as we know this is not the cause of the pain.) Occasionally a scan may be used to help spot arthritis or a stress fracture.
Non Surgical Treatment
If you develop heel pain, you can try several methods at home to ease your discomfort. For example rest as much as possible, apply ice to the heel for 10 to 15 minutes twice a day, use over-the-counter pain medications, wear shoes that fit properly, wear night splints, a special device that stretches the foot while you sleep, use heel cups or shoe inserts to reduce pain, If these home care strategies do not ease your pain, you will need to see your doctor. He or she will perform a physical exam and ask you about your symptoms and when they began. Your doctor may also take an X-ray to determine the cause of your heel pain. Once your doctor knows what is causing your pain, he or she will be able to provide you with the appropriate treatment. In many cases, your doctor may prescribe physical therapy. This can help to strengthen the muscles and tendons in your foot, which helps to prevent further injury. If your pain is severe, your doctor may provide you with anti-inflammatory medications. These medications can be injected into the foot or taken by mouth. Your doctor may also recommend that you support your foot as much as possible-either by taping the foot or by using special footwear devices. In very rare cases, your doctor may recommend surgery to correct the problem. However, heel surgery often requires a long recovery time and may not always relieve your foot pain.
Surgical Treatment
Surgery to correct heel pain is generally only recommended if orthotic treatment has failed. There are some exceptions to this course of treatment and it is up to you and your doctor to determine the most appropriate course of treatment. Following surgical treatment to correct heel pain the patient will generally have to continue the use of orthotics. The surgery does not correct the cause of the heel pain. The surgery will eliminate the pain but the process that caused the pain will continue without the use of orthotics. If orthotics have been prescribed prior to surgery they generally do not have to be remade.
Prevention
Maintaining flexible and strong muscles in your calves, ankles, and feet can help prevent some types of heel pain. Always stretch and warm-up before exercising. Wear comfortable, properly fitting shoes with good arch support and cushioning. Make sure there is enough room for your toes.
Achilles Tendon Pain Treatment And Cause
Overview
 Achilles tendinitis can be a very crippling issue for runners - simply because the pain is enough to discourage loading of the foot. It can also be a tricky condition to treat because the tendon is not as heavily vascularized (i.e. more blood flow) as muscle, and therefore lacks healing potential. It is highly recommended that you see a physical therapist as soon as you experience acute symptoms, so chronic tendonosis (which is longer termed and harder to treat) does not set in.
Achilles tendinitis can be a very crippling issue for runners - simply because the pain is enough to discourage loading of the foot. It can also be a tricky condition to treat because the tendon is not as heavily vascularized (i.e. more blood flow) as muscle, and therefore lacks healing potential. It is highly recommended that you see a physical therapist as soon as you experience acute symptoms, so chronic tendonosis (which is longer termed and harder to treat) does not set in.
Causes
Tendons are the tough fibres that connect muscle to bone. Most tendon injuries occur near joints, such as the shoulder, elbow, knee, and ankle. A tendon injury may seem to happen suddenly, but usually it is the result of many tiny tears to the tendon that have happened over time. Health professionals may use different terms to describe a tendon injury. You may hear, Tendonitis (or Tendinitis): This actually means "inflammation of the tendon," but inflammation is rarely the cause of your tendon pain.
Symptoms
Signs and symptoms of Achilles Tendinitis generally include pain and stiffness along your achilles tendon, especially in the morning. Pain in the back of your heel that gets worse with activity. Severe pain the day after exercising. Swelling that gets worse with activity. If you feel a pop in the back of your heel or bottom of you calf, you may have ruptured or torn you achilles tendon.
Diagnosis
Examination of the achilles tendon is inspection for muscle atrophy, swelling, asymmetry, joint effusions and erythema. Atrophy is an important clue to the duration of the tendinopathy and it is often present with chronic conditions. Swelling, asymmetry and erythema in pathologic tendons are often observed in the examination. Joint effusions are uncommon with tendinopathy and suggest the possibility of intra-articular pathology. Range of motion testing, strength and flexibility are often limited on the side of the tendinopathy. Palpation tends to elicit well-localized tenderness that is similar in quality and location to the pain experienced during activity. Physical examinations of the Achilles tendon often reveals palpable nodules and thickening. Anatomic deformities, such as forefoot and heel varus and excessive pes planus or foot pronation, should receive special attention. These anatomic deformities are often associated with this problem. In case extra research is wanted, an echography is the first choice of examination when there is a suspicion of tendinosis. Imaging studies are not necessary to diagnose achilles tendonitis, but may be useful with differential diagnosis. Ultrasound is the imaging modality of first choice as it provides a clear indication of tendon width, changes of water content within the tendon and collagen integrity, as well as bursal swelling. MRI may be indicated if diagnosis is unclear or symptoms are atypical. MRI may show increased signal within the Achilles.
Nonsurgical Treatment
Relieving the stress is the first course of action. Treatment involves ice therapy and activity modification to reduce inflamation. Active stretching and strengthening exercises will assist rehabilitation of the gastrocnemius-soleus complex. When placed in a heeled shoe, the patient will immediately notice a difference, compared to flat ground. It is recommended that the patient be fitted with proper shoes & orthotics to control pronation and maintain proper alignment, relieving the stress on the achilles tendon. Tightness in the tendon itself can be helped by an extra heel lift added to the orthotics. The patient can expect a slow recovery over a period of months.

Surgical Treatment
The type of surgery you will have depends on the type of injury you are faced with. The longer you have waited to have surgery will also be a factor that determines what type of surgery is needed. With acute (recent) tearing the separation in your Achilles tendon is likely to be very minimal. If you have an acute tear you may qualify for less invasive surgery (such as a mini-open procedure). Surgeons will always choose a shorter, less invasive procedure if it is possible to do so. Most surgeons know that a less complicated procedure will have less trauma to the tendon and a much quicker rate of recovery after the surgery.
Prevention
If you're just getting started with your training, be sure to stretch after running, and start slowly, increasing your mileage by no more than 10% per week. Strengthen your calf muscles with exercises such as toe raises. Work low-impact cross-training activities, such as cycling and swimming, into your training.
Achilles tendinitis can be a very crippling issue for runners - simply because the pain is enough to discourage loading of the foot. It can also be a tricky condition to treat because the tendon is not as heavily vascularized (i.e. more blood flow) as muscle, and therefore lacks healing potential. It is highly recommended that you see a physical therapist as soon as you experience acute symptoms, so chronic tendonosis (which is longer termed and harder to treat) does not set in.
Causes
Tendons are the tough fibres that connect muscle to bone. Most tendon injuries occur near joints, such as the shoulder, elbow, knee, and ankle. A tendon injury may seem to happen suddenly, but usually it is the result of many tiny tears to the tendon that have happened over time. Health professionals may use different terms to describe a tendon injury. You may hear, Tendonitis (or Tendinitis): This actually means "inflammation of the tendon," but inflammation is rarely the cause of your tendon pain.
Symptoms
Signs and symptoms of Achilles Tendinitis generally include pain and stiffness along your achilles tendon, especially in the morning. Pain in the back of your heel that gets worse with activity. Severe pain the day after exercising. Swelling that gets worse with activity. If you feel a pop in the back of your heel or bottom of you calf, you may have ruptured or torn you achilles tendon.
Diagnosis
Examination of the achilles tendon is inspection for muscle atrophy, swelling, asymmetry, joint effusions and erythema. Atrophy is an important clue to the duration of the tendinopathy and it is often present with chronic conditions. Swelling, asymmetry and erythema in pathologic tendons are often observed in the examination. Joint effusions are uncommon with tendinopathy and suggest the possibility of intra-articular pathology. Range of motion testing, strength and flexibility are often limited on the side of the tendinopathy. Palpation tends to elicit well-localized tenderness that is similar in quality and location to the pain experienced during activity. Physical examinations of the Achilles tendon often reveals palpable nodules and thickening. Anatomic deformities, such as forefoot and heel varus and excessive pes planus or foot pronation, should receive special attention. These anatomic deformities are often associated with this problem. In case extra research is wanted, an echography is the first choice of examination when there is a suspicion of tendinosis. Imaging studies are not necessary to diagnose achilles tendonitis, but may be useful with differential diagnosis. Ultrasound is the imaging modality of first choice as it provides a clear indication of tendon width, changes of water content within the tendon and collagen integrity, as well as bursal swelling. MRI may be indicated if diagnosis is unclear or symptoms are atypical. MRI may show increased signal within the Achilles.
Nonsurgical Treatment
Relieving the stress is the first course of action. Treatment involves ice therapy and activity modification to reduce inflamation. Active stretching and strengthening exercises will assist rehabilitation of the gastrocnemius-soleus complex. When placed in a heeled shoe, the patient will immediately notice a difference, compared to flat ground. It is recommended that the patient be fitted with proper shoes & orthotics to control pronation and maintain proper alignment, relieving the stress on the achilles tendon. Tightness in the tendon itself can be helped by an extra heel lift added to the orthotics. The patient can expect a slow recovery over a period of months.
Surgical Treatment
The type of surgery you will have depends on the type of injury you are faced with. The longer you have waited to have surgery will also be a factor that determines what type of surgery is needed. With acute (recent) tearing the separation in your Achilles tendon is likely to be very minimal. If you have an acute tear you may qualify for less invasive surgery (such as a mini-open procedure). Surgeons will always choose a shorter, less invasive procedure if it is possible to do so. Most surgeons know that a less complicated procedure will have less trauma to the tendon and a much quicker rate of recovery after the surgery.
Prevention
If you're just getting started with your training, be sure to stretch after running, and start slowly, increasing your mileage by no more than 10% per week. Strengthen your calf muscles with exercises such as toe raises. Work low-impact cross-training activities, such as cycling and swimming, into your training.
What Will Cause Painful Heel To Flare Up
Overview
Heel pain is most commonly caused by plantar fasciitis, which is the swelling of the tissue that connects the heel bone to the toes at the bottom part of the foot, also known as the plantar fascia. Plantar fasciitis is often described as sharp pain in the middle of the heel, which is typically worse after periods of rest when fascia contracts. The pain usually becomes more bearable as the muscles loosen up during the low-impact walking, but can return even worse after extended periods of walking or standing. The plantar fascia serves as a shock absorber and supports the foot’s arch. Too much tension on the plantar fascia can cause inflammation and swelling. Fortunately in most cases, plantar fasciitis treatment is fairly conservative. Plantar fasciitis exercises, medications and orthotics are usually all that’s needed to manage the pain. Most severe cases may require surgery.
Causes
Training on improper, hard and/or irregular surfaces as well as excessive track work in spiked shoes, or steep hill running, can stress the plantar fascia past its limits of elasticity, leading to injury. Finally, failure in the early season to warm up gradually gives the athlete insufficient time for the structures of the foot to re-acclimate and return to a proper fitness level for intensive exercise. Such unprepared and repeated trauma causes microscopic tearing, which may only be detected once full-blown plantar fasciitis and accompanying pain and debilitation have resulted. If the level of damage to the plantar fascia is significant, an inflammatory reaction of the heel bone can produce spike-like projections of new bone, known as heel spurs. Indeed, plantar fasciitis has occasionally been refereed to as heel spur syndrome, though such spurs are not the cause of the initial pain but are instead a further symptom of the problem. While such spurs are sometimes painless, in other cases they cause pain or disability in the athlete, and surgical intervention to remove them may be required. A dull, intermittent pain in the heel is typical, sometimes progressing to a sharp, sustained discomfort. Commonly, pain is worse in the morning or after sitting, later decreasing as the patient begins walking, though standing or walking for long periods usually brings renewal of the pain.
Symptoms
When plantar fasciitis occurs, the pain is typically sharp and usually unilateral (70% of cases).Heel pain worsens by bearing weight on the heel after long periods of rest. Individuals with plantar fasciitis often report their symptoms are most intense during their first steps after getting out of bed or after prolonged periods of sitting. Improvement of symptoms is usually seen with continued walking. Numbness, tingling, swelling, or radiating pain are rare but reported symptoms. If the plantar fascia continues to be overused in the setting of plantar fasciitis, the plantar fascia can rupture. Typical signs and symptoms of plantar fascia rupture include a clicking or snapping sound, significant local swelling, and acute pain in the sole of the foot.
Diagnosis
Your doctor will ask you about the kind of pain you're having, when it occurs and how long you've had it. If you have pain in your heel when you stand up for the first time in the morning, you may have plantar fasciitis. Most people with plantar fasciitis say the pain is like a knife or a pin sticking into the bottom of the foot. After you've been standing for a while, the pain becomes more like a dull ache. If you sit down for any length of time, the sharp pain will come back when you stand up again.
Non Surgical Treatment
First check your shoes for too much midfoot flexibility and check your training for changes. A detailed evaluation of changes in your training is necessary. You should start with what is called "relative rest" which means a decrease in workout intensity, duration of session and decrease in the number of sessions per week. The most important part of self treatment for this condition is being sure that your shoes offer sufficient stability and are optimal in controlling the forces that contribute to plantar fasciitis and heel spurs. Check your running shoes to make sure that they are not excessively worn. They should bend only at the ball of the foot, where your toes attach to the foot. This is vital! Avoid any shoe that bends in the center of the arch or behind the ball of the foot. It offers insufficient support and will stress your plantar fascia. The human foot was not designed to bend here and neither should a shoe be designed to do this. You should also be doing gentle calf stretching exercises. This will reduce stress on the plantar fascia in two ways. The first manner in which a relaxation of the tension in the calf muscles can help heel pain is that it will reduce the direct pull backwards on the heel bone (calcaneus). The second reason is a little bit more complicated, but essentially it is that a tight achilles tendon and calf muscles causes the rearfoot to move in a manner that causes over pronation as your leg and body move forward over your foot. So go ahead and gently stretch the calf muscle by doing the runner's wall leaning stretch. To strengthen the muscles in your arch toe curls or "doming" can be done. Toe curls may be done by placing a towel on a kitchen floor and then curling your toes to pull the towel towards you. This exercise may also be done without the towel against the resistance of the floor.

Surgical Treatment
In unusual cases, surgical intervention is necessary for relief of pain. These should only be employed after non-surgical efforts have been used without relief. Generally, such surgical procedures may be completed on an outpatient basis in less than one hour, using local anesthesia or minimal sedation administrated by a trained anesthesiologist. In such cases, the surgeon may remove or release the injured and inflamed fascia, after a small incision is made in the heel. A surgical procedure may also be undertaken to remove bone spurs, sometimes as part of the same surgery addressing the damaged tissue. A cast may be used to immobilize the foot following surgery and crutches provided in order to allow greater mobility while keeping weight off the recovering foot during healing. After removal of the cast, several weeks of physical therapy can be used to speed recovery, reduce swelling and restore flexibility.
What Leads To Heel Discomfort And The Way To Cure It

Overview
Heel pain is most often caused by plantar fasciitis, a condition that is sometimes also called heel spur syndrome when a spur is present. Heel pain may also be due to other causes, such as a stress fracture, tendonitis, arthritis, nerve irritation, or, rarely, a cyst. Because there are several potential causes, it is important to have heel pain properly diagnosed. A foot and ankle surgeon is able to distinguish between all the possibilities and determine the underlying source of your heel pain. Plantar fasciitis is an inflammation of the band of tissue (the plantar fascia) that extends from the heel to the toes. In this condition, the fascia first becomes irritated and then inflamed, resulting in heel pain.
Causes
Plantar Fasciitis is simply caused by overstretching of the plantar fascia ligament under the foot. So why is the ligament being overstretched? There are different factors, over-use, too much sports, running, walking or standing for long periods (e.g. because of your job) weight gain, our feet are designed to carry a 'normal' weight. Any excess weight places great pressure on the bones, nerves, muscles and ligaments in the feet, which sooner or later will have consequences. Even pregnancy (in the last 10 weeks) can cause foot problems! age, as we get older ligaments become tighter & shorter and msucles become weaker; the ideal circumstances for foot problems, unsupportive footwear, 'floppy' shoes with no support as well as thongs affect our walking pattern, walking barefoot, especially on hard surfaces like concrete or tiles, low arch and flat feet or over-pronation. An important contributing factor to Plantar Fasciitis is 'excess pronation' (or over-pronation). This is a condition whereby the feet roll over, the arches collapse and the foot elongates. This unnatural elongation puts excess strain on the ligaments, muscles and nerves in the foot. When the foot is not properly aligned, the bones unlock and cause the foot to roll inward. With every step taken your foot pronates and elongates, stretching the plantar fascia and causing inflammation and pain at the attachment of the plantar fascia into the heel bone. Re-alignment of the foot should therefore an important part of the treament regime.
Symptoms
Plantar fasciitis which usually occurs on one foot at a time typically develops slowly. Some cases can be sudden and severe. If you suspect that you have plantar fasciitis, you should feel a sharp, stabbing heel pain, usually in the inside bottom part of the heel. The pain will likely be worse when you take the first steps after long periods of rest (especially after sleep). The pain may also worsen as you stand, climb stairs, or tiptoe. You typically will not feel a lot of pain during exercise, but will feel the ache after. In some cases, the affected heel may even swell.
Diagnosis
After you describe your symptoms and discuss your concerns, your doctor will examine your foot. Your doctor will look for these signs. A high arch, an area of maximum tenderness on the bottom of your foot, just in front of your heel bone. Pain that gets worse when you flex your foot and the doctor pushes on the plantar fascia. The pain improves when you point your toes down. Limited "up" motion of your ankle. Your doctor may order imaging tests to help make sure your heel pain is caused by plantar fasciitis and not another problem. X-rays provide clear images of bones. They are useful in ruling out other causes of heel pain, such as fractures or arthritis. Heel spurs can be seen on an x-ray. Other imaging tests, such as magnetic resonance imaging (MRI) and ultrasound, are not routinely used to diagnose plantar fasciitis. They are rarely ordered. An MRI scan may be used if the heel pain is not relieved by initial treatment methods.
Non Surgical Treatment
Treatment for plantar fasciitis should begin with rest, icing, and over the counter medications. As mentioned above, an orthotic is a device that can be slipped into any pair of shoes and can often relieve pain and help to reverse the damage and occurrence of plantar fasciitis. They do this by adding support to the heel and helping to distribute weight during movement. In addition to orthotics, many people consider night splints for treating this condition. These devices are worn during the night while you sleep, helping to keep the plantar fascia stretched to promote healing. Physical therapy has also become a common option. With this conservative treatment alternative, a physical therapist designs a set of exercises that are intended to address your specific needs in order to promote healing.

Surgical Treatment
Surgery is rarely needed in the treatment of plantar fasciitis. The vast majority of patients diagnosed with plantar fasciitis will recover given ample time. With some basic treatment steps, well over 90% of patients will achieve full recovery from symptoms of plantar fasciitis within one year of the onset of treatment. Simple treatments include anti-inflammatory medication, shoe inserts, and stretching exercises. In patients where a good effort with these treatments fails to provide adequate relief, some more aggressive treatments may be attempted. These include cortisone injections or extracorporeal shock wave treatments.
Prevention
Do your best to maintain healthy weight. Plantar fasciitis is caused by wear and tear on your feet. Being overweight drastically increases the pounding your feet take every day. Even losing a few pounds can help reduce heel pain. Avoid jobs that require walking or standing for long periods of time. Having your body weight on your feet all day puts a lot of pressure on your plantar fascia tissue. Replace your shoes on a regular basis. Buy new shoes when the old ones are worn-out. Make sure your shoes will fit your foot size comfortably at the end of the day. Pay attention to the width as well as the length. Use good supportive shoes that will help you with your original problem like arch support, motion control, stability, cushioning etc. Stretch regularly as part of your daily routine. There are a few special stretching techniques for the prevention. Choose soft surfaces for your exercise routine to walk, jog or run on. Rest and elevate your feet every chance you have. Strengthen your foot muscles as part of your exercise routine. Strong foot muscles provide a good support to the plantar fascia. Change your shoes during the work week. Don't wear the same pair of shoes every day. Perform Warm up exercises such as a short period of walking, a light jog or other easy movement and then stretch before starting the main exercise. Try to avoid dramatic changes in your exercise routine. Increase your exercise level gradually. Don’t run long distance if you are used to walk. Make the change slowly and gradually. Pay attention to your foot pain, do not ignore it. Visit your doctor if the pain continues. Avoid the activities that cause you pain. Use over-the-counter Orthotics or inserts that your doctor may prescribe. Off-the-shelf or custom-fitted arch supports (orthotics) will help distribute pressure to your feet more evenly. Try to avoid barefoot walking, since it may add stress on the plantar fascia ligament.
What Brings About Plantar Fasciitis To Flare Up

Overview
Plantar fasciitis is the most common cause of pain on the bottom of the heel. Approximately 2 million patients are treated for this condition every year. Plantar fasciitis occurs when the strong band of tissue that supports the arch of your foot becomes irritated and inflamed. The plantar fascia is a long, thin ligament that lies directly beneath the skin on the bottom of your foot. It connects the heel to the front of your foot, and supports the arch of your foot.
Causes
Your plantar fascia (fay-sha) supports the arch of your foot as you run or walk. It is a thick, inelastic, fibrous band that starts in your heel, runs along the bottom of your foot, and spreads out to your toes. Plantar fasciitis is an inflammation of this fibrous band. If you are female or have a job that requires a lot of walking or standing on hard surfaces you are more at risk for plantar fasciitis. Additional causes include Being overweight, Having flat feet or high arches, Wearing shoes with poor support, Walking or running for exercise, Tight calf muscles that limit how far you can flex your ankles, Running on soft terrain, Increase in activity level, Genetic predisposition.
Symptoms
Plantar fasciosis is characterized by pain at the bottom of the heel with weight bearing, particularly when first arising in the morning; pain usually abates within 5 to 10 min, only to return later in the day. It is often worse when pushing off of the heel (the propulsive phase of gait) and after periods of rest. Acute, severe heel pain, especially with mild local puffiness, may indicate an acute fascial tear. Some patients describe burning or sticking pain along the plantar medial border of the foot when walking.
Diagnosis
Your doctor will check your feet and watch you stand and walk. He or she will also ask questions about your past health, including what illnesses or injuries you have had. Your symptoms, such as where the pain is and what time of day your foot hurts most. How active you are and what types of physical activity you do. Your doctor may take an X-ray of your foot if he or she suspects a problem with the bones of your foot, such as a stress fracture.
Non Surgical Treatment
First check your shoes for too much midfoot flexibility and check your training for changes. A detailed evaluation of changes in your training is necessary. You should start with what is called "relative rest" which means a decrease in workout intensity, duration of session and decrease in the number of sessions per week. The most important part of self treatment for this condition is being sure that your shoes offer sufficient stability and are optimal in controlling the forces that contribute to plantar fasciitis and heel spurs. Check your running shoes to make sure that they are not excessively worn. They should bend only at the ball of the foot, where your toes attach to the foot. This is vital! Avoid any shoe that bends in the center of the arch or behind the ball of the foot. It offers insufficient support and will stress your plantar fascia. The human foot was not designed to bend here and neither should a shoe be designed to do this. You should also be doing gentle calf stretching exercises. This will reduce stress on the plantar fascia in two ways. The first manner in which a relaxation of the tension in the calf muscles can help heel pain is that it will reduce the direct pull backwards on the heel bone (calcaneus). The second reason is a little bit more complicated, but essentially it is that a tight achilles tendon and calf muscles causes the rearfoot to move in a manner that causes over pronation as your leg and body move forward over your foot. So go ahead and gently stretch the calf muscle by doing the runner's wall leaning stretch. To strengthen the muscles in your arch toe curls or "doming" can be done. Toe curls may be done by placing a towel on a kitchen floor and then curling your toes to pull the towel towards you. This exercise may also be done without the towel against the resistance of the floor.

Surgical Treatment
Surgery for plantar fasciitis can be very successful in the right patients. While there are potential complications, about 70-80% of patients will find relief after plantar fascia release surgery. This may not be perfect, but if plantar fasciitis has been slowing you down for a year or more, it may well be worth these potential risks of surgery. New surgical techniques allow surgery to release the plantar fascia to be performed through small incisions using a tiny camera to locate and cut the plantar fascia. This procedure is called an endoscopic plantar fascia release. Some surgeons are concerned that the endoscopic plantar fascia release procedure increases the risk of damage to the small nerves of the foot. While there is no definitive answer that this endoscopic plantar fascia release is better or worse than a traditional plantar fascia release, most surgeons still prefer the traditional approach.
Stretching Exercises
In one exercise, you lean forward against a wall with one knee straight and heel on the ground. Your other knee is bent. Your heel cord and foot arch stretch as you lean. Hold for 10 seconds, relax and straighten up. Repeat 20 times for each sore heel. It is important to keep the knee fully extended on the side being stretched. In another exercise, you lean forward onto a countertop, spreading your feet apart with one foot in front of the other. Flex your knees and squat down, keeping your heels on the ground as long as possible. Your heel cords and foot arches will stretch as the heels come up in the stretch. Hold for 10 seconds, relax and straighten up. Repeat 20 times. About 90 percent of people with plantar fasciitis improve significantly after two months of initial treatment. You may be advised to use shoes with shock-absorbing soles or fitted with an off-the-shelf shoe insert device like a rubber heel pad. Your foot may be taped into a specific position. If your plantar fasciitis continues after a few months of conservative treatment, your doctor may inject your heel with steroidal anti-inflammatory medication. If you still have symptoms, you may need to wear a walking cast for two to three weeks or a positional splint when you sleep. In a few cases, surgery is needed for chronically contracted tissue.